

Preterm infants have increased nutrient requirements to achieve the growth velocity of a child growing in its mother’s womb4,5. These requirements are much higher than those of a term born peer4-6. Medical associations such as the European Society for Gastroenterology, Hepatology, and Nutrition (ESPGHAN)6 and American Academy of Pediatrics (AAP)7 as well as neonatal experts⁸ address these requirements by giving specific recommendations for premature infants born weighing less than 1000g, less than 1500g and less than 1800g. All these associations acknowledge that protein is a key nutrient in avoiding growth failure as long as enough energy is provided6-8.
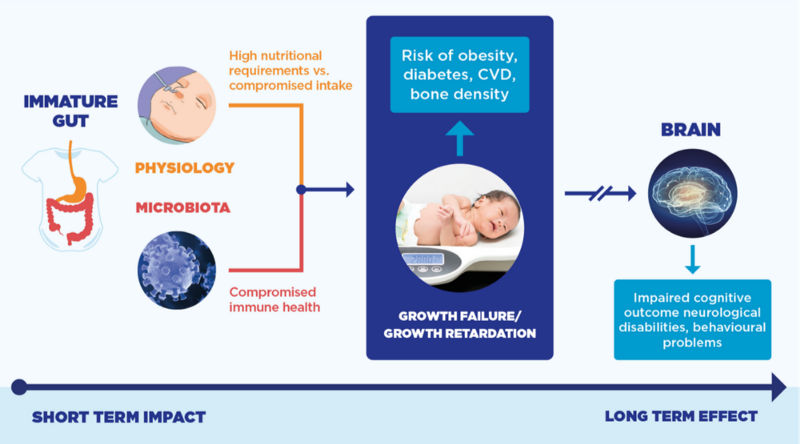
In support of optimal growth and development, preterm nutrition should address:
- High nutritional needs and growth velocity versus difficulties of enteral intake
- Instable metabolsim due to immature gastrointestinal development
- Immature / compromised immune system
- Delayed colonisation and compromised microbiota development
- Sensitive phase of brain development

